Talk:Prostate cancer staging
A fact from Prostate cancer staging appeared on Wikipedia's Main Page in the Did you know column on 1 December 2005. The text of the entry was as follows:
|
| This article is rated Start-class on Wikipedia's content assessment scale. It is of interest to the following WikiProjects: | ||||||||||||||
| ||||||||||||||

Wiki Education Foundation-supported course assignment
![]() This article is or was the subject of a Wiki Education Foundation-supported course assignment. Further details are available on the course page. Student editor(s): Missmaprice, Lhuynh1102.
This article is or was the subject of a Wiki Education Foundation-supported course assignment. Further details are available on the course page. Student editor(s): Missmaprice, Lhuynh1102.
Above undated message substituted from Template:Dashboard.wikiedu.org assignment by PrimeBOT (talk) 07:19, 17 January 2022 (UTC)
Comments
If anyone has any better suggestion for the name of this page, please suggest it. Even if we don't end up moving it, it can redirect here. I'll try to think of good variants to redirect now. — Knowledge Seeker দ 08:06, 28 November 2005 (UTC)
And isn't it a copyright violation to just copy the descriptions from the AJCC recs? I'm unsure how this works; I'll reword the descriptions. — Knowledge Seeker দ 08:13, 28 November 2005 (UTC)
I've got an idea that the outline might be more immediately clear if the initials were included in the header level, so I've put that in, but if you don't like it, feel free to revert. --Arcadian 03:28, 29 November 2005 (UTC)
Here's a suggestion. How about adding a section on prognosis? I realize that prognosis in prostate ca is not straight-forward, but even basics would be helpful. Thanks for your work so far.
Probably not; a prognosis is generally felt to be dangerous by men who have prostate cancer. So much can depend on their attitude, their fitness and their life-style, none of which the medic can really factor in. To be given a prognosis can sound like a sentence of death, and may quash the hope that keeps people going. Better a bromide such as "...we'll keep you going for a long time yet..."
[Note that, for T3/T4 staging, most will survive for many many years, depending on their attitude, fitness etc. Few will actually die within the year, and that may result from other issues with their health, which again is hard for the medic to factor in. For T1/T2, assuming no spread, radical treatment can "cure" (i.e. put into remission) the cancer for the rest of their lives. It can reappear, though.] —Preceding unsigned comment added by 86.1.79.166 (talk) 10:45, 16 February 2010 (UTC)
comments
Medic? It's really work for a doctor to factor in... and this is the best reason to leave it out. Unless... there is some real solid research. This is a page about information, bot about second guessing intentions and playing psychologist. Gingermint (talk) 04:11, 28 September 2010 (UTC)
It is exactly the use of 'bromides' suggested above that demands better information on prognoses and outcomes. Even allowing the dated nature of statistical evidence, the survivability of different staged tumours must be relevent to every sufferer and physician alike. What is the point of having Wikipedia deal with medical issues at all, if science is going to obscure the truth and return us to days when medecine was akin to a 'black art' and only the MD knows best! 86.155.68.178 (talk) 07:25, 30 April 2011 (UTC) Peter Elliott
outdated
All this staging is outdated. Nobody uses 6th ed AJCC anymore. (And, all staging systems are prognostic.) Would be good to add a graphic of national survival curves by stage, as in the AJCC manual. Time to update to AJCC 7th. — Preceding unsigned comment added by Scarbrtj (talk • contribs) 15:20, 12 September 2011 (UTC)
Suggested Edits from QMed
Hello, we are a group of medical students editing this page as part of our class assignment. We have compiled a list of suggestions to improve this article and would appreciate community feedback before we proceed with these edits. Here is a list of our suggestions:
Suggestions:
1) Add a wiki link to the following: PSA, prostate cancer, American Joint Committee on Cancer
2) TNM Staging Section should be updated with references to the 7th edition of AJCC and UICC.[1]. For the T1 description: we suggest that "tumor present, but not detectable clinically or with imaging" should be changed to "tumor present, but not palpable or detectable with imaging".[2]
3) We suggest an edit that will differentiate between clinical and pathological staging more clearly in the beginning by including the definition of each.
Replace: "imaging studies and blood tests (so-called "clinical stage"), or based on the extent of disease as revealed in a surgical specimen (so-called "pathological stage"),
Insert "Prostate cancer stage can be assessed by either clinical or pathological staging methods. Clinical staging usually occurs before the first treatment and tumour presence is determined through imaging and rectal examination, while pathological staging is done after treatment once a biopsy is performed or the prostate is removed by looking at the cell types within the sample".[3]
- Can you replace "prognostic classification" with an easier to understand term?JenOttawa (talk) 13:42, 7 November 2017 (UTC)
- I changed the wording, hopefully this is an improvement
4)Change the sentence "Another scheme, now used less commonly for research, but often still used by clinicians, is the Whitmore-Jewett stage," to "Another scheme that was used in the past was Whitmore-Jewett staging, although TNM staging is more common in modern practice.[4]
Under the Whitmore-Jewett staging section:
*remove: "The Whitmore-Jewett system is similar to the TNM system, with approximately equivalent stages."
*insert: "Although it is no longer commonly used in practice, the Whitmore-Jewett system is similar to the TNM system and has similar stages".[4]
5) Clarify “risk” based on Gleason scale. Add: "A Gleason score of 6 is considered low risk and 3+4=7 is intermediate risk. Both 4+3=7 and 8-10 are considered high risk."[5]
6) Make Gleason Grade consistent throughout. i.e., In the article, it mentions G score, cancer grade, histologic grade, etc. We suggest replacing those with "Gleason Grade". Replace: “G3-4: the tumor resembles normal tissue barely or not at all”, with: "G3-4: the tissue does not appear normal" or "G3-4: the tumor tissue does not resemble normal tissue."[5]
7) Add: "While the utility of absolute PSA values is still controversial (particularly for use in prostate cancer screening) the rate of rise and doubling time of PSA are useful indicators of the aggressiveness of a prostate cancer, and measuring PSA is also widely accepted as a way to monitor patients following their treatment.[6]
- Can you replace "utility" and "aggressiveness" with simple words?JenOttawa (talk) 13:42, 7 November 2017 (UTC)
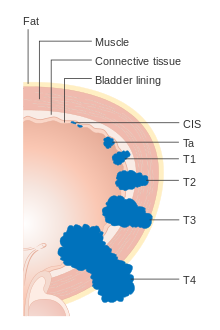
8) Addition of the image following images may help in visualization of the T staging - these images are not copyrighted
a) https://upload.wikimedia.org/wikipedia/commons/thumb/5/5c/Diagram_showing_the_T_stages_of_bladder_cancer_CRUK_372.svg/2000px-Diagram_showing_the_T_stages_of_bladder_cancer_CRUK_372.svg.png --> For the T staging b) https://upload.wikimedia.org/wikipedia/commons/thumb/6/65/Diagram_showing_a_transperineal_prostate_biopsy_CRUK_473.svg/1057px-Diagram_showing_a_transperineal_prostate_biopsy_CRUK_473.svg.png --> For showing how biopsy is done if wanted
9) The wikipage for "prostatic capsule" is no longer there, so instead of a hyperlink, we can define prostatic capule and have the term in brackets in the following manner: "In Stage III, the tumour has spread through a thin layer of connective tissue that envelopes the prostate gland (prostatic capsule) and the lump can be felt on the surface of the gland."[2]
- Have you given some consideration to user RexxS's comments below re the figures? If you need help or more advice, please let me knowJenOttawa (talk) 18:58, 17 November 2017 (UTC)
Thank you so much, we appreciate any feedback you may have for us! Danielle, Meg, Madison, Louis, Wasim, Emma Drobi036 (talk) 20:04, 5 November 2017 (UTC)
References
- ^ ...], American Joint Committee on Cancer. [Ed.: Stephen B. Edge (2010). AJCC cancer staging manual (7th ed. ed.). New York: Springer. ISBN 9780387884400.
{{cite book}}:|edition=has extra text (help);|last1=has numeric name (help) - ^ a b "TNM | UICC". www.uicc.org.
- ^ Cheng, Liang; Montironi, Rodolfo; Bostwick, David G.; Lopez-Beltran, Antonio; Berney, Daniel M. (January 2012). "Staging of prostate cancer". Histopathology. 60 (1): 87–117. doi:10.1111/j.1365-2559.2011.04025.x. ISSN 1365-2559. PMID 22212080.
- ^ a b Williamson, edited by Phillip Bennett, Catherine (2010). Basic science in obstetrics and gynaecology : a textbook for MRCOG Part I (4th ed. ed.). Edinburgh: Churchill Livingstone. p. 322. ISBN 978-0443102813.
{{cite book}}:|edition=has extra text (help);|first1=has generic name (help)CS1 maint: multiple names: authors list (link) - ^ a b Cosma, G; Acampora, G; Brown, D; Rees, RC; Khan, M; Pockley, AG (2016). "Prediction of Pathological Stage in Patients with Prostate Cancer: A Neuro-Fuzzy Model". PloS one. 11 (6): e0155856. doi:10.1371/journal.pone.0155856. PMID 27258119.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ Laposata, [edited by] Michael (2014). Laboratory medicine (Second edition. ed.). ISBN 9780071805544.
{{cite book}}:|first1=has generic name (help)
- COMMENTS: Little things - In the book references, when you fill in the number for the edition the template automatically adds "ed." so you have "edition ed." or "ed. ed." Book citations need page numbers. Something wrong at the beginning of the first citation, and the second citation needs more description of what it is. Speaking of which, is UICC a reputable organization? Can you use your ref for American Joint Committee on Cancer instead? David notMD (talk) 15:38, 8 November 2017 (UTC)
- Comments:

- Adding wikilinks is almost always helpful; check you've read WP:OVERLINK for when it's not recommended.
- When you update to a later edition of a resource, you need to check that the article text is still supported by the newer edition. Amend it if necessary, and don't forget to update page numbers if they have changed.
- Your suggestion gives a clearer indication to me about the difference between the clinical and pathological staging, so is an improvement. Remember that your audience is a lay reader, so try to avoid WP:JARGON as much as possible. See if you can address Jenny's comment about "prognostic classification".
- Are you sure that the Whitmore-Jewett system is no longer commonly used in practice? or is it simply less commonly used? Please be clear about what the sources say.
- I don't think that your suggestion about risk,
Example text
reads clearly at all. Please have another think about what you're trying to say and re-phrase it. Perhaps "A Gleason score of 6 is considered low risk and 3+4=7 is intermediate risk. Both 4+3=7 and 8-10 are considered high risk." might be clearer? - We should only use terms as they are used in the sources, but where it is clear that something like "G score" means "Gleason score", then that sort of change is reasonable. Make sure you keep the distinction between Gleason score and Gleason grade where it is significant.
- The note about utility of absolute PSA values is useful.
- Explaining specialised terms like prostatic capsule is useful, whether there is an article available to link to or not. Worth doing.
- The images – I've used the standard syntax to demonstrate to you – look better than File:Diagram showing T1-3 stages of prostate cancer CRUK 278.svg and File:Prostate Needle Biopsy.png to me, so you'd have my support for replacing them. However, there's an OTRS ticket shown for File:Diagram showing the T stages of bladder cancer CRUK 372.svg, but you will probably need to also have one for File:Diagram showing a transperineal prostate biopsy CRUK 473.svg, given the claim by the uploader that it's their work.
- Here are the references reformatted as I would write them:
- American Joint Committee on Cancer (2010). Edge, Stephen B (ed.). AJCC cancer staging manual (7th ed.). New York: Springer. pp. ??. ISBN 9780387884400.
– you must supply page numbers for books! - "What is TNM?". Union for International Cancer Control. 2017. Retrieved 11 November 2017.
- Cheng, Liang; Montironi, Rodolfo; Bostwick, David G; Lopez-Beltran, Antonio; Berney, Daniel M (January 2012). "Staging of prostate cancer". Histopathology. 60 (1): 87–117. doi:10.1111/j.1365-2559.2011.04025.x. ISSN 1365-2559. PMID 22212080.
- Williamson, Catherine (2010). Bennett, Phillip (ed.). Basic science in obstetrics and gynaecology: a textbook for MRCOG, Part I (4th ed.). Edinburgh: Churchill Livingstone. p. 322. ISBN 978-0443102813.
- Cosma, G; Acampora, G; Brown, D; Rees, RC; Khan, M; Pockley, AG (2016). "Prediction of Pathological Stage in Patients with Prostate Cancer: A Neuro-Fuzzy Model". PloS one. 11 (6): e0155856. doi:10.1371/journal.pone.0155856. PMC 4892614. PMID 27258119.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - Laposata, Michael, ed. (2014). Laboratory medicine: the diagnosis of disease in the clinical laboratory (Second ed.). McGraw Hill. p. 371–376. ISBN 9780071805544.
– I couldn't find the phrase "PSA value". You must supply page numbers (and preferably chapter numbers for compendium books, as individual chapters have different authors).
- American Joint Committee on Cancer (2010). Edge, Stephen B (ed.). AJCC cancer staging manual (7th ed.). New York: Springer. pp. ??. ISBN 9780387884400.
- That's not to say you must use exactly that style; most editors develop their own quirks. Nevertheless, references to books must include page numbers – you can't expect readers to search through an entire book to find your source. Page numbers are usually unnecessary for journal articles, and obviously not used for webpages. Hope that helps. --RexxS (talk) 17:42, 11 November 2017 (UTC)
- Thank you for your suggestions RexxS; we will definitely take your suggestions into consideration and edit our changes before inserting into the wiki page. We had an in class session in which we discussed Prostate Staging with a urologist, and he confirmed the WJ Staging is no longer used in clinic and is an archaic staging form. We will read over the 'Overlink' page, find our page numbers, and re-format the wording for some of our changes. Thank you so much!

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Drobi036 (talk) 18:29, 11 November 2017 (UTC)
- Why is UICC described in text as 7th edition? David notMD (talk) 01:18, 16 November 2017 (UTC)
- We did not cite the new 8th edition for UICC for Prostate Cancer TNM staging because it has made certain changes that are no longer compatible with AJCC's 7th edition. For example, 8th edition of UICC shows that Stage III of the overall staging now includes T4, N0, M0 whereas in the 7th edition, it is still part of stage IV. The 8th edition of AJCC comes out in January 2018, but until then we are basing most of the TNM staging on AJCC's 7th edition, and using UICC 7th edition to support it. Drobi036 (talk) 16:25, 18 November 2017 (UTC)
- Why is UICC described in text as 7th edition? David notMD (talk) 01:18, 16 November 2017 (UTC)