Spermatocele
| Spermatocele | |
|---|---|
| Other names: Spermatic cyst,[1] epididymal cyst, testicular cyst[2] | |
 | |
| Ultrasound of a testicle (grey) and a spermatocele (black). | |
| Pronunciation | |
| Specialty | Urology |
| Symptoms | Scrotal mass, testicular pain[1] |
| Usual onset | 40s and 50s[2] |
| Causes | Unknown[5] |
| Diagnostic method | Examination, ultrasound[6] |
| Differential diagnosis | Hydrocele, inguinal hernia, testicular cancer, varicocele, lymphedema[6] |
| Treatment | None, aspiration, sclerotherapy, or surgery[1] |
| Frequency | Up to 30% of males[2] |
Spermatocele is a fluid-filled cyst in the epididymis.[7] They occur behind or above the testicle.[2] They vary in size from millimeters to a few centimeters.[2] They are generally not painful; though some have a dull ache.[1] They are not associated with infertility.[2]
The cause is unknown.[5] Proposed possibilities include injury, infection, and inflammation.[5] The fluid they contain is usually milky colored and contain sperm.[5] Diagnosis is based on examination and sometimes ultrasound.[6] They are not cancer, nor do they increase the risk of testicular cancer.[1]
They rarely require specific treatment.[1] If pain occurs acetaminophen or ibuprofen may be used.[1] Occasionally procedures such as aspiration or sclerotherapy, or surgery may be done.[1] Spermatoceles occur in up to 30% males.[2] They are more common in those in their 40s and 50s.[2]
Causes
Spermatoceles can originate as diverticulum from the tubules found in the head of the epididymis. Sperm accumulation gradually causes the diverticulum to increase in size, causing a spermatocele. Since there are many tubules connecting the epididymis to the testis, a blockage in one of the tubules may lead to formation of a cyst.[8] In many instances they appear to occur spontaneously without any preceding instances of injury.[2]
Scarring of any part of the epididymis due to trauma or inflammation can cause it to become obstructed and in turn form a spermatocele.[9]
Risk factors
It is not well known what may be causing the growth of a spermatocele. It has been observed that pregnant women who were prescribed diethylstilbestro (DES) to prevent pregnancy complications, such as miscarriage, and gave birth to a son most likely increased the risk of the son to develop a spermatocele in the future. However, doctors stopped prescribing this medication in 1971 since it increased the risk of women developing a rare vaginal cancer.[10]
Children
Epididymal cysts may arise in children due to numerous different reasons. They may even originate from a disturbance in endocrine factors during the development of the embryo.[11] The incidence of these cysts are possibly linked to boys who are exposed to diethylstilbestrol, an estrogen medication, while in the fetus.[11]
Although the evidence and information for incidence of spermatoceles in children is lacking, there are general management guidelines for caregivers who may encounter spermatoceles in their children.[12] Epididymal cysts are typically benign in nature. However, caregivers should take note of any discomfort and symptoms in children, including but not limited to, erythema, scrotal edema or swelling.[12] Epididymal cysts appear in approximately 70% of boys who present as asymptomatic.[12] The diagnosis of epididymal cysts in children can be discovered upon physical examination and eventually confirmed via ultrasound.[12]
Anatomy

Spermatoceles are important to not be ignored as it can affect the male reproductive system. The testes are organs inside the scrotum that create sperm as well as sex hormones and testosterone. The sperm in the testes move to the epididymis which is a long, coiled tube behind the testes. The primary function is to store and mature sperm so it can fertilize the egg. However, if the epididymis becomes injured, then there is a chance that the sperm will not mature and a man will not be able to reproduce with a woman. Therefore, serious thought must be considered when undergoing spermatocelectomy.[13]
Diagnosis
Spermatoceles can be discovered as incidental scrotal masses found on physical examination by a physician or by self-inspection of the scrotum and testicles.[14] The various types of diagnosis for spermatocele types include hydrocele, varicocele, hernia, simple epididymal cyst, and neoplasm.[15]
The primary care physician may diagnose and manage benign causes of scrotal masses such as hydrocele, varicocele and spermatocele. However, if a "must not miss" diagnoses related to testicular masses such as testicular torsion, epididymitis, acute orchitis, strangulated hernia and testicular cancer is suspected, the family physician must refer to a urologist.[16] Finding a painless, cystic mass at the head of the epididymis that is clearly separate from the testicle can indicate a spermatocele. Shining a light through the mass through a process known as transillumination can also help differentiate between a fluid-filled cyst and a tumor, which would not allow as much light to pass.[17] If uncertainty exists, ultrasonography of the scrotum can confirm the presence of a spermatocele.[14] The location and history of any scrotal masses are crucial in determining whether or not the mass is benign or malignant.[18] Lab tests such as a complete blood count (CBC test) or urine test can also be conducted to check for any possible infection or signs of inflammation.[19]
Spermatoceles come in varying sizes and shapes. Some spermatoceles are very small and can only be detected through an ultrasound. More commonly seen are spermatoceles that are a pea-sized lump. They tend to form above or behind a testicle and have a shape and size that looks like a pea. Larger growths have been reported to look similar to a third testicle and can be very discomforting.[19] For those who are affected with large spermatoceles, some have reported feeling pain, heaviness, and fullness in the affected testicle.[17]
If a person is experiencing pain and/or swelling in the scrotum or if a person notices a physical difference such as a mass during a testicular self-exam then they must seek medical attention to help rule out any other causes and begin treatment.[17]
-

Epididymal cyst illuminated by a flashlight
-

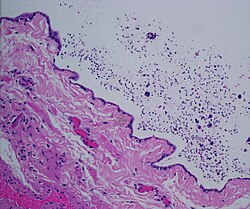
Micrograph of a spermatocele. The characteristic sperm are present (black dots - left of image). H&E stain.
-
Dilated rete testis containing spermatozoa within cyst lumen. H&E stain 20x



Prevention
There is no way to prevent a spermatocele from forming, but there are routines that can be established to help identify any changes in a person's scrotum such as masses, abnormalities, or discomfort. Performing a monthly testicular self-exam can improve the person's chances of identifying spermatoceles or any abnormalities quickly.
It is best to perform a testicular self-exam after a warm shower to help the scrotum relax. To properly exam the scrotum, look for any swelling on the skin and examine each testicle by rolling the testicle between the thumbs and the fingers. A normal testicle is oval-shaped and will usually feel smooth and firm. It is also not uncommon for the testicles to be different sizes.[9]
Upon physical examination, if a 'lump' is found during the testicular exam, further screening may be performed via ultrasound to eliminate testicular cancer.[8]
Treatment
Small cysts as well as asymptomatic larger cysts are better left and carefully observed. However, treatment can be considered if the cysts are causing discomfort, enlarging in size, or per patient request. There are a few different treatment options.[14]
Medications
Certain drugs such as oral analgesics or anti-inflammatory medications can be taken by mouth to decrease spermatocele-related symptoms such as pain and/or swelling. At the moment, there is no medication that can inhibit the production of a spermatocele or cure it. Common medications recommended by doctors are acetaminophen (Tylenol) that can treat pain. To treat the inflammation and pain, non-steroidal anti-inflammatory drugs (NSAIDs) are recommended such as ibuprofen (Motrin, Advil), naproxen (Aleve), and others.[17] Antibiotics may also be prescribed in cases where risk of infection and discomfort is indicated.[15]
Procedures
Aspiration and sclerotherapy are treatments that remove fluid from the spermatocele and seal the spermatocele sac closed from further fluid build-up, respectively.[14] Due to a higher risk of epididymis damage, fertility problems, and further recurrences, these procedures are not recommended and not commonly used.
Surgery
Surgical treatments must be thoroughly discussed with people prior to any final decisions. Different types of surgical procedures may be chosen based on the extent of risk.[20]
A short procedure called a spermatocelectomy can be performed for spermatoceles that cause irritating symptoms. This standard procedure can be performed in an outpatient setting with the use of local or general anesthesia. This procedure typically consists of removing the spermatocele and a portion of the epididymis.[14] The risk of epididymal injury is 17.12%. This incident may happen when the spermatocele is being dissected from the head of the epididymis.[2] Spermatocelectomy can cause complications such as hematoma, wound infection, scrotal abscess as well as recurrence.[15] After surgery, the doctor may recommend to apply ice packs for several days to help reduce swelling. Oral pain medications can also be taken for a few days to reduce discomfort.[14] In addition, the patient returns 2-6 weeks after to inspect any progress/complications.[15] If received a vasectomy, then two semen samples must be collected and analyzed after 6-12 weeks post-operation and several ejaculations. The centrifuged semen samples are used to look for the absence of viable sperm in the semen.[21]
Complications
After surgical removal, it is possible that the pain will persist and recurrence can occur. Fertility may be compromised with these surgical procedures, so people may consider postponing surgery until after having children.[17] If the pain is intolerable and the person would like to get the spermatocele removed immediately, the person should talk to his doctor about the possibility of freezing or donating sperm in case infertility occurs.[22]
Epidemiology
Spermatoceles usually affect men who are middle-aged and can, although rarely, affect children during puberty.[23] The incidence rate is around 5-20% for children.[24] It is estimated that approximately 30 percent of men have been diagnosed with small spermatoceles while less have larger spermatoceles. The incidence of spermatoceles increases as men age.[25] Before puberty, children from the male sex may develop a similar benign mass called epididymis cyst. Although both epididymis cyst and spermatocele may be referred as the same, the epididymis cyst does not contain sperm and it can occur anywhere within the epididymis. It can be differentiated through an ultrasound imagining. Epididymis cysts larger than 10mm in diameter are recommended for surgery but if there is no problem then surgery is discouraged as it can affect fertility in the future.[11]
History
"Spermatocele" is originally derived from the Greek term spermatos (sperm) and kele (cavity or mass).[15] Often times, "epididymal cyst" has been used interchangeably with "spermatocele." However, it is important to note their differences. Epididymal cysts may appear anywhere along or within the epididymis and do not contain sperm, whereas spermatoceles may contain sperm. Epididymal cysts have been shown to occur more frequently in children before reaching puberty.[12]
See also
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 "Spermatoceles: Symptoms, Diagnosis & Treatment - Urology Care Foundation". www.urologyhealth.org. Archived from the original on 8 April 2019. Retrieved 13 February 2022.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 "Spermatocele: Symptoms, Causes, Treatments". Cleveland Clinic. Archived from the original on 2020-07-28. Retrieved 2020-07-28.
- ↑ Entry "spermatocele" Archived 2022-02-09 at the Wayback Machine in Merriam-Webster Online Dictionary Archived 2017-09-22 at the Wayback Machine.
- ↑ OED 2nd edition, 1989.
- ↑ 5.0 5.1 5.2 5.3 Rioja, Jorge; Sánchez-Margallo, Francisco M.; Usón, Jesús; Rioja, Luis A. (2011). "Adult hydrocele and spermatocele". BJU International. 107 (11): 1852–1864. doi:10.1111/j.1464-410X.2011.10353.x. ISSN 1464-410X. Archived from the original on 2021-07-29. Retrieved 2021-12-09.
- ↑ 6.0 6.1 6.2 "Scrotal Swelling - Kidney and Urinary Tract Disorders". Merck Manuals Consumer Version. Archived from the original on 20 December 2021. Retrieved 13 February 2022.
- ↑ "Scrotal Swelling - Kidney and Urinary Tract Disorders". Merck Manuals Consumer Version. Archived from the original on 20 December 2021. Retrieved 13 February 2022.
- ↑ 8.0 8.1 "Spermatocele". The Urology Group of Virginia. Archived from the original on 2021-08-02. Retrieved 2021-08-02.
- ↑ 9.0 9.1 "Spermatocele - Symptoms and causes". Mayo Clinic. Archived from the original on 2017-07-29. Retrieved 2020-07-28.
- ↑ "Spermatocele". www.mayoclinic.org. Archived from the original on 2021-07-29. Retrieved 2021-08-01.
- ↑ 11.0 11.1 11.2 Boscarelli, Alessandro; Bellini, Tommaso (2021). "Epididymal cyst in children". European Journal of Pediatrics. doi:10.1007/s00431-021-04080-5. ISSN 1432-1076. Archived from the original on 2022-02-09. Retrieved 2021-12-09.
- ↑ 12.0 12.1 12.2 12.3 12.4 Boscarelli, Alessandro; Bellini, Tommaso (2021). "Epididymal cyst in children". European Journal of Pediatrics. doi:10.1007/s00431-021-04080-5. ISSN 1432-1076. Archived from the original on 2022-02-09. Retrieved 2021-12-09.
- ↑ "Male Reproductive System: Structure & Function". Cleveland Clinic. Archived from the original on 2021-12-31. Retrieved 2021-08-01.
- ↑ 14.0 14.1 14.2 14.3 14.4 14.5 "Spermatoceles: Symptoms, Diagnosis & Treatment - Urology Care Foundation". www.urologyhealth.org. Archived from the original on 2019-04-08. Retrieved 2020-07-28.
- ↑ 15.0 15.1 15.2 15.3 15.4 "Spermatocele: Practice Essentials, History of the Procedure, Problem". 2021. Archived from the original on 2021-07-29. Retrieved 2021-12-09.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Junnila, Jennifer; Lassen, Patrick (1998). "Testicular Masses". American Family Physician. 57 (4): 685. ISSN 0002-838X. Archived from the original on 2021-07-28. Retrieved 2021-12-09.
- ↑ 17.0 17.1 17.2 17.3 17.4 "Spermatocele - Diagnosis and treatment - Mayo Clinic". www.mayoclinic.org. Archived from the original on 2021-08-01. Retrieved 2021-08-01.
- ↑ Lee, Jerry C.; Bhatt, Shweta; Dogra, Vikram S. (2008). "Imaging of the Epididymis". Ultrasound Quarterly. 24 (1): 03–16. doi:10.1097/RUQ.0b013e318168f116. ISSN 0894-8771. Archived from the original on 2022-02-09. Retrieved 2021-12-09.
- ↑ 19.0 19.1 "Spermatocele: Symptoms, Causes, Treatments". Cleveland Clinic. Archived from the original on 2020-07-28. Retrieved 2021-08-01.
- ↑ Stuckmann, G (2006). "Sonographie des Skrotums". Praxis. 95 (18): 709–720. doi:10.1024/0369-8394.95.18.709. ISSN 1661-8157. Archived from the original on 2021-08-02. Retrieved 2021-12-09.
- ↑ Kliesch, S. (2014). "[Hydrocele, spermatocele, and vasectomy: management of complications]". Der Urologe. Ausg. A. 53 (5): 671–675. doi:10.1007/s00120-014-3486-4. ISSN 1433-0563. PMID 24806800. Archived from the original on 2021-07-28. Retrieved 2021-12-09.
- ↑ "Spermatocele Disease Reference Guide". Drugs.com. Archived from the original on 2021-07-29. Retrieved 2021-08-01.
- ↑ "Epididymal Cysts. Be clear about Epididymal Cysts. Patient". patient.info. Archived from the original on 2021-07-29. Retrieved 2021-07-29.
- ↑ Bleve, Cosimo; Conighi, Maria Luisa; Bucci, Valeria; Costa, Lorenzo; Chiarenza, Salvatore Fabio (2018). "Torsion of huge epididymal cyst in a 16-year-old boy: case report and review of the literature". La Pediatria Medica E Chirurgica: Medical and Surgical Pediatrics. 40 (1). doi:10.4081/pmc.2018.162. ISSN 2420-7748. PMID 29871476. Archived from the original on 2021-07-29. Retrieved 2021-12-09.
- ↑ "UroPartners - Spermatoceles". uropartners.com. Archived from the original on 2019-04-08. Retrieved 2021-07-29.
External links
| Classification |
|---|