Polymorphic eruption of pregnancy
| Polymorphic eruption of pregnancy | |
|---|---|
| Other names: Pruritic urticarial papules and plaques of pregnancy (PUPPP) | |
 | |
| Typical rash of PEP presenting along the stretch marks | |
| Specialty | Dermatology, obstetrics |
| Symptoms | Itchy hives, small blisters, widespread redness with clearing around the belly button[1] |
| Complications | No long-term risks for mother or baby[2] |
| Usual onset | Late pregnancy or shortly after childbirth[1] |
| Duration | 4 to 6 weeks[3] |
| Causes | Unclear[1] |
| Risk factors | First pregnancy, larger belly, multiple pregnancies[1] |
| Differential diagnosis | Pemphigus gestationis, prurigo of pregnancy, pruritic folliculitis of pregnancy, scabies[3] |
| Treatment | Steroid cream, antihistamines[4][3] |
| Prognosis | Resolves after delivery[4] |
| Frequency | 1 in 120 to 300 pregnant women[1] |
Polymorphic eruption of pregnancy (PEP), also known as pruritic urticarial papules and plaques of pregnancy (PUPPP), is the most common specific skin condition of pregnancy.[1][2] Symptoms include very itchy hives, small blisters, and widespread redness with a non-involved area around the belly button.[1] It often first appear within stretch marks before before spreading to the thighs and trunk; while the face and upper chest is not generally involved.[1][4] Onset is typically in the later part of pregnancy or shortly after childbirth.[1]
It most commonly affects women in their first pregnancy, those with larger bellies, and those carrying multiple pregnancies.[1] While the underlying mechanism is unclear it may involve skin stretching.[1] Diagnosis can often be based on symptoms.[3] Generally, lab tests are normal, except for occasionally an increase in IgE.[3]
Treatment is with corticosteroids.[4] Generally these are applied to the skin such as betamethasone valerate 0.1%; though may occasionally be taken by mouth.[4][3] Antihistamines, like cetirizine, may also be used.[3] The condition resolves after delivery.[4] It presents no long-term risks for either the mother or baby.[2] It is unusual for it to reoccur.[2]
Polymorphic eruption of pregnancy affects 1 in 120 to 300 pregnant women.[1] In those with twins or triplets 3 to 17% are affected.[2] Those affected are may be twice as likely to be carrying a male baby.[2] The condition was first described in 1979.[4]
Signs and Symptoms
PEP most commonly presents as a rash that starts within the stretch marks. This rash may then move to other areas of the body, including, but not limited to the trunk of the body, arms, legs, feet, chest, and neck. Very few people experiencing PUPPP have reported the rash spreading to the face, palms of hands, or soles of feet.[5]
This rash usually begins with the skin looking abnormally red and feeling itchy, accompanied by notable swelling of skin tissue that appears raised and within the stretch marks.[6][7] Over time, individual segments of this rash can join to form one whole, larger rash with the same characteristics. As this happens, people report noticing the skin surrounding the rash to appear white in color (blanched) and in the shape of "halos". Multiple features of the disease can continue with time and have been reported as widespread erythema (a red skin rash due to damage of underlying capillaries) and patches of inflamed, itchy, rough, and cracked patches of skin that appear similarly to eczema.[7] Other features have been reported in some cases of those experiencing PUPPP, such as tiny vesicles, however these are not as common and develop after more time.
Certain reports have shown there is a positive correlation between PUPPP and excessive maternal weight gain along with increased newborn birth weight. Additionally, a study from Ghazeeri and al. showed that 89% of people who underwent conception through in vitro fertilization were Rh-positive.[8]
The timeline of onset for these symptoms has been reported with some variability. However, most people report experiencing symptoms during the third trimester (last few weeks of pregnancy) where 15% of the women who have PUPPP reported that symptoms actually began immediately after delivery of the baby.[9][10] As mentioned above, the papules and plaques usually first appear on the abdomen (although not on the umbilicus/belly button) and often spread to the legs, chest, underarms, etc. However, lesions on or above the breasts are rare. That's why the face is usually spared and does not become affected. As a result of these papules and plaques from PUPPP, it causes the skin to be very itchy (pruritic) and immensely affects the patient's sleep quality throughout the night.[11]
-

Left side view of abdomen
-

-

-

-
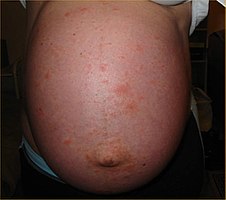
Front view of abdomen
-

Side view of abdomen

.jpg)
.jpg)
.jpg)


Cause
PUPPP is the most common dermatosis of pregnancy and is the most frequent in pregnant women habitating a male fetus, women who had quick and conspicuous weight gain during a short period, and women who ultimately deliver by a c-section.[12][13][14] Although the exact cause of the condition is not known and varying amongst individuals, there have been theories linking the cause of PUPPP to hormonal alterations, damage to the connective tissue during pregnancy, and autoimmune disorder where the evidence for these theories is currently low.[15][16]
This skin condition occurs mostly in first pregnancies (primigravida), in the third trimester and is more likely with multiple pregnancies (more so with triplets than twins or singletons).[17][16][18] Estimated 75% of people with typical PUPPP people have never given birth. Occasionally, this condition may also occur postpartum, but rarely does this ever occur in the first and second trimester.[5][19]
Other than additional associations with hypertension and induction of labour, there are no observed difference in the outcome of the pregnancy for mothers or babies.[20]
Skin diseases
During pregnancy as the abdominal wall rapid stretching, it is hypothesized that there is an inflammatory reaction that occurs due to the exposure of collagen.[9] This reaction has been seen more frequently in those who are having twins or triplets compared to those with single births. This is hypothesized to be due to increased stretching of the abdominal wall while carrying twins or triplets, causing an earlier onset of PUPPP when compared to those undergoing single births.[16][9][21]
Hormones
Throughout pregnancy, there are hormonal changes that occur where it has been hypothesized that these changes may contribute to the onset of PUPPP. Although current research is low on this hypothesis, it has been seen that those who have had multiple gestations can exhibit an increased level of progesterone. With this increase in progesterone, it causes there to be an increased level of progesterone receptors present eliciting an immune reaction seen by skin lesions in PUPPP.[22][23] With multiple gestations, there is an increase in sex hormones that has been seen those with the condition such as an increase in progesterone as previously discussed but also higher levels of estradiol.[24][25] Currently evidence is weak in the role that sex hormones play when contributing to PUPPP where further research is needed.[16]
Immunology
Inflammatory
From those with PUPPP, it has been seen from an immunohistology profile which is used to determine the of tissue components present within an individual via the use of antibodies, that there are certain immune cells that are in greater amount compared to that of those without PUPPP. Immunohistology profile have shown cells consistent with a delayed hypersensitivity with T helper cell infiltrates, dendritic cells and epidermal Langerhans cells.[10]
It has been hypothesized that PUPPP appears in response to fetal antigens that circulate throughout the body. For example, a study showed that fetal male DNA was found within the lesions of the mother's skin which was thought to be caused by the fetal cells seen in the mother's blood throughout pregnancy.[26]
Autoimmune
Although this condition has not been determined as an autoimmune condition, from a single study it has been seen that Immunoglobulin M (IgM) deposition at the dermal-epidermal membrane has been associated with a variety of dermatosis including PUPPP. The problem with the hypothesis that has been proposed is that this condition does not reoccur and it does not progressively worsen.[10] Currently there has been no evidence of detecting circulating antibodies that are associated with the onset on PUPPP in an individual.[22]
Diagnosis

PUPPP is often a diagnosis of exclusion and may need laboratory testing to rule out other dermatoses. Lab tests may include complete blood count, comprehensive metabolic panel, liver function tests, serum human choriogonadotropin and serum cortisol. Additional specialized tests may include serum for indirect immunofluorescence or biopsy of the lesions for direct immunofluorescence to rule out pemphigoid gestationis.[17]
A common misdiagnosis is urticarial pemphigoid gestationis, hence it is needed to exclude it while diagnosing PUPPP as clinical features can overlap. Therefore, histological and immunological studies are necessary to ensure there is no mis-diagnosis. During the case of pemphigoid gestationis, lesions usually occur during the earlier periods of gestation and often involve the umbilicus; as well as, having a positive immunofluorescence of perilesional skin. If there is eczema, people generally have a history of atopy, be it personal or through family. The eruption is identified by pruritic erythematous lesions on flexural areas. Furthermore, other clinical differential diagnosis could be from drug eruptions, urticaria, or viral exanthems.[7]
Sometimes, people may require a 3- or 4-mm punch biopsy to exclude herpes gestationis, which is a variant of bullous pemphigoid occurring during or immediately after pregnancy. Usually the biopsy has features that are consistent with PUPPP but there are no pathognomonic symptoms of the particular disorder. Additionally, a biopsy of unaffected perilesional skin could be used for direct immunofluorescence studies to have a more precise exclusion of herpes gestationis.[27][28]
Treatment
It is important to note that diagnosis should be conducted by a trusted medical professional. In the case that a woman is experiencing symptoms of PUPPP, it is recommended that they contact their primary care physician for referral to a dermatologist for treatment guidance and should not self-treat.[29]
In the majority of cases, PUPPP resolves within a few days or weeks upon initial onset or spontaneously within a week of delivery.[30] However, a few women continue to experience symptoms long into the postpartum period.
One of the most recent forms of treatment suggested is the intramuscular injection of autologous whole blood as an alternative treatment option for people affected by PUPPP right after childbirth, as it seems to have both subjective and objective improvements of the symptoms. This is a very good option for the people who are worried about taking medications during pregnancy or breastfeeding[31]
Antihistamine tablets may be prescribed to provide relief from the itch, although they are generally considered much less effective than corticosteroid treatments,[17] and may decrease itching through blocking histamine release as well as improving sleep quality.
Furthermore, first-generation antihistamines, such as chlorpheniramine, have proven to be safe in pregnancy and can be a supplement treatment for pruritus.[7][32] Second-generation antihistamines such as loratadine and cetirizine are non-sedating and may also be effective in controlling pruritus in pregnant people.[33]
Knowing that oral antihistamines are generally ineffective, high-potency topical steroids are used to treat PUPPP, and ideally tapering it off after 7 days of therapy. Class I or II corticosteroid creams and ointments are used in more aggressive cases, and oral (systemic) corticosteroids can be used to treat very severe cases—although the benefits of a pregnant woman's ingesting high-potency corticosteroids must be weighed carefully against possible (and mostly unknown) risks to the developing fetus or fetuses. The use of high-potency topical corticosteroids over 300 grams throughout the pregnancy may increase the risk of low birth weight for the baby.[34] Rarely, in unusually persistent and distressing cases, some women have had their labor induced as soon as they are considered to be at term (37 weeks).[35]
When the pruritus is unbearable to the patient with PUPPP, oral prednisone in doses of 10 to 40 mg/day has been generally used for these type of severe cases. With this treatment, symptoms are usually relieved after 24 hours of the oral treatment. Sometimes, if the cases are too severe and the symptoms are extremely unbearable, early delivery can be discussed with the patient if the other treatments are ineffective. However, early delivery of the baby still does not guarantee that the symptoms will be gone. Luckily, in most cases, steroid treatment works efficiently and symptoms are generally greatly improved within several days. As with most steroid treatments, the usage of it is a controversial topic. Nonetheless, short-term or one-time use is advisable, and tends to be safer while using it during the third trimester compared to the first trimester.[14]
Pine tar soap/body wash can also bring relief as can keeping the skin chilled such as through a cold shower or iced cloths.
See also
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 Stefaniak, Aleksandra A.; Pereira, Manuel P.; Zeidler, Claudia; Ständer, Sonja (March 2022). "Pruritus in Pregnancy". American Journal of Clinical Dermatology. 23 (2): 231–246. doi:10.1007/s40257-021-00668-7. ISSN 1179-1888. PMC 8860374. PMID 35191007.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Chouk, C; Litaiem, N (January 2023). "Pruritic Urticarial Papules and Plaques of Pregnancy". StatPearls. PMID 30969522. Archived from the original on 25 January 2022. Retrieved 26 December 2023.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 Roth, MM (1 February 2011). "Pregnancy dermatoses: diagnosis, management, and controversies". American journal of clinical dermatology. 12 (1): 25–41. doi:10.2165/11532010-000000000-00000. PMID 21110524.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 James, William D.; Elston, Dirk; Treat, James R.; Rosenbach, Misha A.; Neuhaus, Isaac (2020). "21. Chronic blistering dermatoses". Andrews' Diseases of the Skin: Clinical Dermatology (13th ed.). Edinburgh: Elsevier. p. 465-466. ISBN 978-0-323-54753-6. Archived from the original on 2023-07-01. Retrieved 2023-05-15.
- ↑ 5.0 5.1 Kroumpouzos, George; Cohen, Lisa M. (2003). "Specific dermatoses of pregnancy: An evidence-based systematic review". American Journal of Obstetrics & Gynecology. 188 (4): 1083–1092. doi:10.1067/mob.2003.129. ISSN 0002-9378. PMID 12712115. Archived from the original on 2023-07-01. Retrieved 2023-05-08.
- ↑ Yancey, K. B.; Hall, R. P.; Lawley, T. J. (2003). "Pruritic urticarial papules and plaques of pregnancy. Clinical experience in twenty-five patients". Journal of the American Academy of Dermatology. 10 (3): 473–480. doi:10.1016/s0190-9622(84)80097-3. ISSN 0190-9622. PMID 6725659. Archived from the original on 2022-08-26. Retrieved 2023-05-08.
- ↑ 7.0 7.1 7.2 7.3 Chouk, Chourouk; Litaiem, Noureddine (2021), "Pruritic Urticarial Papules And Plaques Of Pregnancy", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30969522, archived from the original on 25 January 2022, retrieved 29 July 2021
- ↑ Dermatol (2012). "Pruritic urticarial papules and plaques of pregnancy: epidemiological, clinical, and histopathological study of 18 cases from Lebanon". International Journal of Dermatology. 51 (9): 1047–1053. doi:10.1111/j.1365-4632.2011.05203.x. PMID 22909357. S2CID 6347173. Archived from the original on 2022-12-07. Retrieved 2023-05-08.
- ↑ 9.0 9.1 9.2 Bechtel, Mark (2018). "Pruritus in Pregnancy and Its Management". Dermatologic Clinics. 36 (3): 259–265. doi:10.1016/j.det.2018.02.012. ISSN 0733-8635. PMID 29929597. S2CID 49341971. Archived from the original on 2021-08-01. Retrieved 2023-05-08.
- ↑ 10.0 10.1 10.2 Taylor, Drew; Pappo, Eden; Aronson, Iris K. (2016). "Polymorphic eruption of pregnancy". Clinics in Dermatology. 34 (3): 383–391. doi:10.1016/j.clindermatol.2016.02.011. ISSN 1879-1131. PMID 27265077. Archived from the original on 2022-10-04. Retrieved 2023-05-08.
- ↑ Oakley. "Polymorphic eruption of pregnancy". Archived from the original on 2023-03-01. Retrieved 2023-05-08.
- ↑ Shornick, J. K. (2009). "Dermatoses of pregnancy". Seminars in Cutaneous Medicine and Surgery. 17 (3): 172–181. doi:10.1016/s1085-5629(98)80011-4. ISSN 1085-5629. PMID 9759674. Archived from the original on 2023-02-21. Retrieved 2023-05-08.
- ↑ Vaughan Jones, S. A.; Black, M. M. (2002). "Pregnancy dermatoses". Journal of the American Academy of Dermatology. 40 (2 Pt 1): 233–241. doi:10.1016/s0190-9622(99)70194-5. ISSN 0190-9622. PMID 10025751. Archived from the original on 2021-08-02. Retrieved 2023-05-08.
- ↑ 14.0 14.1 Romm (January 2010). "Pregnancy: Third Trimester". CHAPTER 15 - Pregnancy: Third Trimester. Churchill Livingstone. pp. 370–397. doi:10.1016/B978-0-443-07277-2.00017-9. ISBN 9780443072772. Archived from the original on 2021-11-30. Retrieved 2023-05-08.
- ↑ Matz H, Orion E, Wolf R (2006). "Pruritic urticarial papules and plaques of pregnancy: polymorphic eruption of pregnancy (PUPPP)". Clin Dermatol. 24 (2): 105–8. doi:10.1016/j.clindermatol.2005.10.010. PMID 16487883.
- ↑ 16.0 16.1 16.2 16.3 Brzoza, Zenon; Kasperska-Zajac, Alicja; Oleś, Ewa; Rogala, Barbara (2007). "Pruritic urticarial papules and plaques of pregnancy". Journal of Midwifery & Women's Health. 52 (1): 44–48. doi:10.1016/j.jmwh.2006.09.007. ISSN 1542-2011. PMID 17207750. Archived from the original on 2022-06-17. Retrieved 2023-05-08.
- ↑ 17.0 17.1 17.2 Pruritic Urticarial Papules and Plaques of Pregnancy derm/351 at eMedicine
- ↑ Beard, M. P.; Millington, G. W. M. (2012). "Recent developments in the specific dermatoses of pregnancy". Clinical and Experimental Dermatology. 37 (1): 1–5. doi:10.1111/j.1365-2230.2011.04173.x. ISSN 1365-2230. PMID 22007708. S2CID 5428325. Archived from the original on 2021-08-06. Retrieved 2023-05-08.
- ↑ Aronson, I. K.; Bond, S.; Fiedler, V. C.; Vomvouras, S.; Gruber, D.; Ruiz, C. (1998). "Pruritic urticarial papules and plaques of pregnancy: clinical and immunopathologic observations in 57 patients". Journal of the American Academy of Dermatology. 39 (6): 933–939. doi:10.1016/s0190-9622(98)70265-8. ISSN 0190-9622. PMID 9843004. Archived from the original on 2023-04-05. Retrieved 2023-05-08.
- ↑ Ohel I, Levy A, Silberstein T, Holcberg G, Sheiner E (May 2006). "Pregnancy outcome of patients with pruritic urticarial papules and plaques of pregnancy". J Matern Fetal Neonatal Med. 19 (5): 305–8. doi:10.1080/14767050600590573. PMID 16753771. S2CID 20129348.
- ↑ Rimoin, Lauren P.; Kwatra, Shawn G.; Yosipovitch, Gil (2013). "Female-specific pruritus from childhood to postmenopause: clinical features, hormonal factors, and treatment considerations". Dermatologic Therapy. 26 (2): 157–167. doi:10.1111/dth.12034. ISSN 1529-8019. PMID 23551372. S2CID 3500357. Archived from the original on 2022-10-08. Retrieved 2023-05-08.
- ↑ 22.0 22.1 Ahmadi, Sharareh; Powell, Frank C. (2005). "Pruritic urticarial papules and plaques of pregnancy: current status". The Australasian Journal of Dermatology. 46 (2): 53–58, quiz 59. doi:10.1111/j.1440-0960.2005.00160.x. ISSN 0004-8380. PMID 15842394. S2CID 36678742. Archived from the original on 2021-07-29. Retrieved 2023-05-08.
- ↑ Petropoulou, Haritini; Georgala, Sofia; Katsambas, Andreas D. (2006). "Polymorphic eruption of pregnancy". International Journal of Dermatology. 45 (6): 642–648. doi:10.1111/j.1365-4632.2006.02715.x. ISSN 0011-9059. PMID 16796619. S2CID 5718364. Archived from the original on 2022-08-06. Retrieved 2023-05-08.
- ↑ Sävervall, Christine; Sand, Freja Lærke; Thomsen, Simon Francis (2015). "Dermatological Diseases Associated with Pregnancy: Pemphigoid Gestationis, Polymorphic Eruption of Pregnancy, Intrahepatic Cholestasis of Pregnancy, and Atopic Eruption of Pregnancy". Dermatology Research and Practice. 2015: 979635. doi:10.1155/2015/979635. ISSN 1687-6105. PMC 4644842. PMID 26609305.
- ↑ Roth, Maria-Magdalena (2011). "Pregnancy dermatoses: diagnosis, management, and controversies". American Journal of Clinical Dermatology. 12 (1): 25–41. doi:10.2165/11532010-000000000-00000. ISSN 1179-1888. PMID 21110524. S2CID 5181650. Archived from the original on 2022-07-31. Retrieved 2023-05-08.
- ↑ Aractingi, S.; Berkane, N.; Bertheau, P.; Le Goué, C.; Dausset, J.; Uzan, S.; Carosella, E. D. (1998-12-12). "Fetal DNA in skin of polymorphic eruptions of pregnancy". Lancet. 352 (9144): 1898–1901. doi:10.1016/S0140-6736(98)05121-6. ISSN 0140-6736. PMID 9863788. S2CID 22404463. Archived from the original on 2022-06-14. Retrieved 2023-05-08.
- ↑ Fitzpatrick (January 2018). "Urticarial and Indurated Eruptions". Chapter 5 - Urticarial and Indurated Eruptions. Elsevier. pp. 63–82. doi:10.1016/B978-0-323-48553-1.00005-7. ISBN 9780323485531. Archived from the original on 2021-08-02. Retrieved 2023-05-08.
- ↑ Dehdashti (2015). "Pruritic urticarial papules and plaques of pregnancy occurring postpartum". Cutis. 95 (6): 344–347. PMID 26125211. Archived from the original on 2022-10-04. Retrieved 2023-05-08.
- ↑ Kurien, George; Badri, Talel (2021), "Dermatoses of Pregnancy", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28613614, archived from the original on 2020-12-31, retrieved 2021-08-02
- ↑ Brandão, Pedro; Sousa-Faria, Bárbara; Marinho, Carla; Vieira-Enes, Pedro; Melo, Anabela; Mota, Lurdes (February 2017). "Polymorphic eruption of pregnancy: Review of literature". Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology. 37 (2): 137–140. doi:10.1080/01443615.2016.1225019. ISSN 1364-6893. PMID 27960565. S2CID 6034995. Archived from the original on 2022-10-04. Retrieved 2023-05-08.
- ↑ Kim (2017). "Pruritic Urticarial Papules and Plaques of Pregnancy Occurring Postpartum Treated with Intramuscular Injection of Autologous Whole Blood". Case Reports in Dermatology. 9 (1): 151–156. doi:10.1159/000473874. PMC 5437438. PMID 28559815.
- ↑ Schatz, M.; Petitti, D. (2002). "Antihistamines and pregnancy". Annals of Allergy, Asthma & Immunology. 78 (2): 157–159. doi:10.1016/S1081-1206(10)63382-0. ISSN 1081-1206. PMID 9048523. Archived from the original on 2021-08-02. Retrieved 2023-05-08.
- ↑ Källén, B. (2003). "Use of antihistamine drugs in early pregnancy and delivery outcome". The Journal of Maternal-Fetal & Neonatal Medicine. 11 (3): 146–152. doi:10.1080/jmf.11.3.146.152. ISSN 1476-7058. PMID 12380668. S2CID 26679676. Archived from the original on 2022-06-17. Retrieved 2023-05-08.
- ↑ Chi, Ching-Chi; Wang, Shu-Hui; Mayon-White, Richard; Wojnarowska, Fenella (2013). "Pregnancy outcomes after maternal exposure to topical corticosteroids: a UK population-based cohort study". JAMA Dermatology. 149 (11): 1274–1280. doi:10.1001/jamadermatol.2013.5768. ISSN 2168-6084. PMID 24005903.
- ↑ De G, De G (January 2002). "Pruritic urticarial papules and plaques of pregnancy: an unusual case" (PDF). J Am Osteopath Assoc. 102 (1): 44–6. PMID 11837341. Archived from the original (PDF) on 2007-09-27.
External links
| Classification | |
|---|---|
| External resources |
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||