Chronic pancreatitis
| Chronic pancreatitis | |
|---|---|
| Other names: Pancreatitis - chronic - discharge | |
 | |
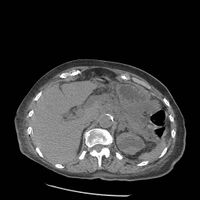
| Axial CT showing multiple calcifications in the pancreas in a patient with chronic pancreatitis | |
| Specialty | Gastroenterology |
| Symptoms | None, abdominal pain, weight loss, vomiting, greasy bad smelling stool[1] |
| Complications | Diabetes, malnutrition, pancreatic pseudocyst, pancreatic cancer[1] |
| Duration | Long-term |
| Causes | Alcoholism, pancreatic duct obstruction, cystic fibrosis, autoimmune pancreatitis, high blood calcium, high blood lipids[1] |
| Diagnostic method | MRCP or ERCP[1] |
| Differential diagnosis | Peptic ulcer disease, gallstones, acute pancreatitis, pancreatic cancer, mesenteric ischemia[1] |
| Prevention | Avoiding alcohol and smoking[1] |
| Treatment | Low fat meals, fat soluble vitamins, pancreatic enzymes, pain medications, surgery[1] |
| Frequency | 6 per 10,000 (USA)[2] |
Chronic pancreatitis is a long-term inflammation of the pancreas that affects its function functions.[1] There is may be periods of no symptoms, though at time abdominal pain may occur.[1] Other symptoms may include weight loss, vomiting, and greasy bad smelling stool.[1] Complications may include diabetes, malnutrition, pancreatic pseudocyst, and pancreatic cancer.[1]
The cause in about 75% of cases is alcoholism.[1][3] Other causes include pancreatic duct obstruction, cystic fibrosis, autoimmune pancreatitis, high blood calcium, certain medications, and high blood lipids.[1] The underlying mechanism may involve either plugs forming within the pancreatic ducts or activation of digestive enzymes within the pancreas.[1] Diagnosis may be supported by MRCP or ERCP with lipase levels often being normal.[1] A stool fat measurement over 72 hours may be useful.[1]
There is no cure.[2] Management may involve eating low fat meals, fat soluble vitamin supplementation, and pancreatic enzymes.[1] People should stop smoking and drinking alcohol.[1] Pain may be treated with tricyclic antidepressants, NSAIDs, or gabapentin.[1] Opioids or surgery may be used if other measures are not effective.[1]
How commonly it occurs is unclear.[1] One estimate from the United States put the frequency at 6 per 10,000.[2] Similar numbers have been found in Europe and Asia.[2] The typical age at diagnosis is 45.[1] Life expectancy may be decreased in those affected.[2] The condition was first described in 1788 by Cawley.[3]
Signs and symptoms
- Upper abdominal pain: Upper abdominal pain which increases after drinking or eating, lessens when fasting or sitting and leaning forward. Some people may not suffer pain.[4]
- Nausea and vomiting[4]
- Steatorrhea: Frequent, oily, foul-smelling bowel movements. Damage to the pancreas reduces the production of pancreatic enzymes that aid digestion, which can result in malnutrition. Fats and nutrients are not absorbed properly, leading to loose, greasy stool known as steatorrhea.[4]
- Weight loss even when eating habits and amounts are normal.
- Diabetes type 1: Chronic pancreatitis can affect the ability of the pancreatic islets to produce insulin to regulate glucose levels, leading to diabetes type 1.[4] Symptoms of diabetes type 1 include increased hunger and thirst, frequent urination, weight loss, and fatigue.[citation needed]
Causes
Among the causes of chronic pancreatitis are the following:[5]
- Alcohol
- Autoimmune disorders
- Intraductal obstruction
- Idiopathic pancreatitis
- Tumors
- Ischemia
- Calcific stones
The relationship between etiologic factors, genetic predisposition, and the pace of disease progression requires further clarification, though recent research indicates smoking may be a high-risk factor to develop chronic pancreatitis.[6] In a small group of patients chronic pancreatitis has been shown to be hereditary. Almost all patients with cystic fibrosis have established chronic pancreatitis, usually from birth. Cystic fibrosis gene mutations have also been identified in patients with chronic pancreatitis but in whom there were no other manifestations of cystic fibrosis. Obstruction of the pancreatic duct because of either a benign or malignant process may result in chronic pancreatitis.[7]
Pathophysiology

The mechanism of chronic pancreatitis viewed from a genetic standpoint indicates early onset of severe epigastric pain beginning in childhood. It is an autosomal dominant disease, chronic pancreatitis disease is identified in the cationic trypsinogen gene PRSS1, and mutation, R122H. R122H is the most common mutation for hereditary chronic pancreatitis with replacement of arginine with histidine at amino acid position 122 of the trypsinogen protein. There are, of course, other mechanisms – alcohol, malnutrition, smoking – each exhibiting its own effect on the pancreas.[8]
Diagnosis
The diagnosis of chronic pancreatitis is based on tests on pancreatic structure and function. Serum amylase and lipase may be moderately elevated in cases of chronic pancreatitis. A secretin stimulation test is considered the best test for diagnosis of chronic pancreatitis. Other tests used to determine chronic pancreatitis are serum trypsinogen, computed tomography, ultrasound and biopsy.[9][10]
When chronic pancreatitis is caused by genetic factors, elevations in ESR, IgG4, rheumatoid factor, ANA and anti-smooth muscle antibody may be detected.[11]
On CT scan, pancreatic and bile duct dilatation, atropy of pancreas, multiple calcifications of the pancreas, and enlargement of pancreatic glands can be found.[12]
On MRI scan, there is a low T1 signal due to inflammation, fibrosis, focal lesions, and calcifications. In those who are given with a contrast agent, there would be a higher T1 signal with late gadolinium enhancement due to compression from the fibrotic areas. The overall thickness of the pancreas will be reduced. Magnetic resonance cholangiopancreatography (MRCP) is the most useful option in accessing the pancreatic duct and bile duct.[12]
-
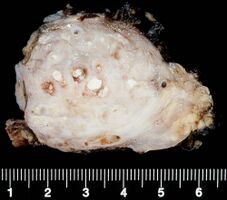
Chronic pancreatitis
-

Chronic calcific pancreatitis
-

Acute on chronic pancreatitis
-
Acute on chronic pancreatitis
_(Radiopaedia_27870).jpeg)
.jpg)
.JPG)
.jpg)
Treatment
The different treatment options for management of chronic pancreatitis are medical measures, therapeutic endoscopy and surgery.[13] Treatment is directed, when possible, to the underlying cause, and to relieve pain and malabsorption. Insulin dependent diabetes mellitus may occur and need long-term insulin therapy.[14] The abdominal pain can be very severe and require high doses of analgesics, sometimes including opiates. Alcohol cessation and dietary modifications (low-fat diet) are important to manage pain and slow the calcific process.[13] Antioxidants may help but it is unclear if the benefits are meaningful.[15]
Pancreatic enzymes
Pancreatic enzyme replacement is often effective in treating the malabsorption and steatorrhea associated with chronic pancreatitis. Treatment of CP consists of administration of a solution of pancreatic enzymes with meals. Some patients do have pain reduction with enzyme replacement and since they are relatively safe, giving enzyme replacement to a chronic pancreatitis patient is an acceptable step in treatment for most patients. Treatment may be more likely to be successful in those without involvement of large ducts and those with idiopathic pancreatitis.[16]
Surgery
Surgery to treat chronic pancreatitis tends to be divided into two areas – resectional and drainage procedures. Among the reasons to opt for surgery are if there is a pseudocyst, fistula, ascites, or a fixed obstruction.[5]
Epidemiology
The annual incidence of chronic pancreatitis is 5 to 12 per 100,000 persons, the prevalence is 50 per 100,000 persons.[17]
See also
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 1.15 1.16 1.17 1.18 1.19 1.20 1.21 Benjamin, O; Lappin, SL (January 2020). "Chronic Pancreatitis". PMID 29493950.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ 2.0 2.1 2.2 2.3 2.4 Beyer, G; Habtezion, A; Werner, J; Lerch, MM; Mayerle, J (15 August 2020). "Chronic pancreatitis". Lancet (London, England). 396 (10249): 499–512. doi:10.1016/S0140-6736(20)31318-0. PMID 32798493.
- ↑ 3.0 3.1 Wilson, Peter; Watson, Paul; Haythornwaite, Jennifer; Jensen, Troels (2008). Clinical Pain Management : Chronic Pain. CRC Press. p. 553. ISBN 978-1-4441-0981-8. Archived from the original on 2021-08-28. Retrieved 2021-02-14.
- ↑ 4.0 4.1 4.2 4.3 "What is chronic pancreatitis?". Archived from the original on 2017-05-09. Retrieved 2017-02-07.
diabetes; upper abdominal pain that is frequently chronic and debilitating. Pain is the most common symptom of chronic pancreatitis. The pain may increase after drinking or eating, and lessens when fasting or sitting and leaning forward. However, some people with chronic pancreatitis report little to no pain; from google (chronic pancreatitis smelly poop) result 1
- ↑ 5.0 5.1 "Chronic Pancreatitis: Practice Essentials, Background, Pathophysiology". 2018-11-11. Archived from the original on 2015-11-08. Retrieved 2015-11-29.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Tolstrup, J. S.; Kristiansen, L.; Becker, U.; Grønbaek, M. (2009). "Smoking and Risk of Acute and Chronic Pancreatitis Among Women and Men". Archives of Internal Medicine. 169 (6): 603–609. doi:10.1001/archinternmed.2008.601. PMID 19307524.
- ↑ Choices, NHS. "Chronic pancreatitis - Causes - NHS Choices". www.nhs.uk. Archived from the original on 2015-12-08. Retrieved 2015-11-29.
- ↑ Brock, Christina; Nielsen, Lecia Møller; Lelic, Dina; Drewes, Asbjørn Mohr (2013-11-14). "Pathophysiology of chronic pancreatitis". World Journal of Gastroenterology. 19 (42): 7231–7240. doi:10.3748/wjg.v19.i42.7231. ISSN 1007-9327. PMC 3831204. PMID 24259953.
- ↑ "Chronic Pancreatitis. Hereditary pancreas disorders information | Patient". Patient. Archived from the original on 2015-11-28. Retrieved 2015-11-29.
- ↑ "Acute Pancreatitis. Pancreatitis Symptoms and Information | Patient". Patient. Archived from the original on 2015-12-08. Retrieved 2015-11-29.
- ↑ Kapural, Leonardo (2014-12-03). Chronic Abdominal Pain: An Evidence-Based, Comprehensive Guide to Clinical Management. Springer. p. 91. ISBN 9781493919925. Archived from the original on 2016-06-23. Retrieved 2015-11-29.
- ↑ 12.0 12.1 Kamat, Rohan; Gupta, Pankaj; Rana, Surinder (2019-04-01). "Imaging in chronic pancreatitis: State of the art review". Indian Journal of Radiology and Imaging. 29 (2): 201. doi:10.4103/ijri.IJRI_484_18. ISSN 0971-3026. PMID 31367093. Archived from the original on 2020-07-08. Retrieved 2020-07-07.
- ↑ 13.0 13.1 American Gastroenterological Association Medical Position Statement (1998). "American Gastroenterological Association Medical Position Statement: treatment of pain in chronic pancreatitis". Gastroenterology. 115 (3): 763–4. doi:10.1016/S0016-5085(98)70156-8. PMID 9721174. – via ScienceDirect (Subscription may be required or content may be available in libraries.)|Available online 27 October 2005
- ↑ Ewald, Nils; Hardt, Philip D (2013-11-14). "Diagnosis and treatment of diabetes mellitus in chronic pancreatitis". World Journal of Gastroenterology. 19 (42): 7276–7281. doi:10.3748/wjg.v19.i42.7276. ISSN 1007-9327. PMC 3831209. PMID 24259958.
- ↑ Ahmed Ali, U; Jens, S; Busch, OR; Keus, F; van Goor, H; Gooszen, HG; Boermeester, MA (Aug 21, 2014). "Antioxidants for pain in chronic pancreatitis" (PDF). The Cochrane Database of Systematic Reviews. 8 (8): CD008945. doi:10.1002/14651858.CD008945.pub2. PMID 25144441. Archived (PDF) from the original on April 27, 2019. Retrieved January 7, 2019.
- ↑ Sikkens, E. C. M.; Cahen, D. L.; Kuipers, E. J.; Bruno, M. J. (2010-06-01). "Pancreatic enzyme replacement therapy in chronic pancreatitis". Best Practice & Research. Clinical Gastroenterology. 24 (3): 337–347. doi:10.1016/j.bpg.2010.03.006. ISSN 1532-1916. PMID 20510833. – via ScienceDirect (Subscription may be required or content may be available in libraries.)
- ↑ Yadav, Dhiraj; Lowenfels, Albert B. (2013-06-01). "The Epidemiology of Pancreatitis and Pancreatic Cancer". Gastroenterology. 144 (6): 1252–1261. doi:10.1053/j.gastro.2013.01.068. ISSN 0016-5085. PMC 3662544. PMID 23622135.
Further reading
- Yan, M‐X; Li, Y‐Q (2006-04-01). "Gall stones and chronic pancreatitis: the black box in between". Postgraduate Medical Journal. 82 (966): 254–258. doi:10.1136/pgmj.2005.037192. ISSN 0032-5473. PMC 2579631. PMID 16597812.
- Lerch, Markus M.; Gorelick, Fred S. (2013). "Models of Acute and Chronic Pancreatitis". Gastroenterology. 144 (6): 1180–1193. doi:10.1053/j.gastro.2012.12.043. PMID 23622127. Archived from the original on 2021-08-28. Retrieved 2015-11-29.
External links
| Classification | |
|---|---|
| External resources |