Pulmonary edema
| Pulmonary edema | |
|---|---|
| Other names: Pulmonary oedema | |
 | |
| Pulmonary edema with small pleural effusions on both sides. | |
| Specialty | Cardiology, critical care medicine |
| Symptoms | Shortness of breath, lung crackles, pink frothy sputum[1] |
| Complications | Respiratory failure[1] |
| Types | Cadiogenic, non-cardiogenic[1] |
| Causes | Cardiogenic: Heart attack, myocarditis, valvular heart disease, heart arrythmias[1] Non-cardiogenic: Acute respiratory distress syndrome (ARDS), pneumonia, pancreatitis, multiple blood transfusions[1] |
| Diagnostic method | Supported by lab tests and medical imaging[1] |
| Treatment | Cardiogenic: Furosemide, nitroglycerin, non-invasive ventilation[2] Non-cardiogenic: Oxygen therapy, mechanical ventilation[3] |
| Frequency | Relatively common[4] |
Pulmonary edema is fluid accumulation in the tissue and air spaces of the lungs.[1] Symptoms may include shortness of breath, lung crackles, and pink frothy sputum.[1] Complications may include respiratory failure.[1]
It may occur due to heart failure (cardiogenic) or injury to the lung tissue (non-cardiogenic pulmonary edema).[1] Heart failure may occur due to a heart attack, myocarditis, valvular heart disease, or heart arrythmias.[1] Lung injury may been seen with acute respiratory distress syndrome (ARDS) and result from pneumonia, pancreatitis, or multiple blood transfusions.[1] The underlying mechanism involves impaired gas exchange.[1] Diagnosis may be supported by lab tests and medical imaging.[1]
Treatment is focused on improving symptoms and addressing the underlying cause.[1] Additional efforts in cardiogenic pulmonary edema may involve diuretics such as furosemide, efforts to decrease afterload such as nitroglycerin, and non-invasive ventilation.[2] Additional efforts in non-cardiogenic pulmonary edema involves supportive care such as oxygen therapy and mechanical ventilation.[3]
Pulmonary edema is relatively common.[4] Cardiogenic cases affects more than a million people a year in the United States while non-cardiogenic cases affect about 190,000.[1] The risk of death when hospitalized has decreased from 60% in 1970s to 30% in the 1990s.[1] Pulmonary edema has been described since at least the time of Hippocrates around 400 BC.[5] The term edema is from the Greek οἴδημα (oídēma) meaning "swelling".[6]
Signs and symptoms
The most common symptom of pulmonary edema is difficulty breathing, but may include other symptoms such as coughing up blood (classically seen as pink, frothy sputum), excessive sweating, anxiety, and pale skin. Shortness of breath can manifest as orthopnea (inability to lie down flat due to breathlessness) and/or paroxysmal nocturnal dyspnea (episodes of severe sudden breathlessness at night). These are common presenting symptoms of chronic pulmonary edema due to left ventricular failure. The development of pulmonary edema may be associated with symptoms and signs of "fluid overload"; this is a non-specific term to describe the manifestations of right ventricular failure on the rest of the body and includes peripheral edema (swelling of the legs, in general, of the "pitting" variety, wherein the skin is slow to return to normal when pressed upon), raised jugular venous pressure and hepatomegaly, where the liver is enlarged and may be tender or even pulsatile. Other signs include end-inspiratory crackles (sounds heard at the end of a deep breath) on auscultation and the presence of a third heart sound.[7]
Cause
Classically it is cardiogenic (left ventricular) but fluid may also accumulate due to damage to the lung. This damage may be direct injury or injury mediated by high pressures within the pulmonary circulation. When directly or indirectly caused by increased left ventricular pressure pulmonary edema may form when mean pulmonary pressure rises from the normal of 15 mmHg[8] to above 25 mmHg.[9] Broadly, the causes of pulmonary edema can be divided into cardiogenic and non-cardiogenic. By convention cardiogenic refers to left ventricular causes.
Cardiogenic
- Congestive heart failure which is due to the heart's inability to pump the blood out of the pulmonary circulation at a sufficient rate resulting in elevation in wedge pressure and pulmonary edema – this may be due to left ventricular failure, arrhythmias, or fluid overload, e.g., from kidney failure or intravenous therapy.
- Hypertensive crisis can cause pulmonary edema as the elevation in blood pressure and increased afterload on the left ventricle hinders forward flow and causes the elevation in wedge pressure and subsequent pulmonary edema.
Non-cardiogenic
- Negative pressure pulmonary edema[10] in which a significant negative pressure in the chest (such as from an inhalation against an upper airway obstruction) ruptures capillaries and floods the alveoli. Negative pressure pulmonary edema has an incidence in the range of 0.05-0.1% for general anesthesia. The negative pressure causes a significant increase in preload, thereby increasing pulmonary blood volume. There is also a significant increase in left ventricular afterload, which causes a decreased cardiac output. The increase in pulmonary blood volume along with a decrease in cardiac output will increase the pulmonary transudative pressures. With all this occurring, pulmonary vascular resistance increases causing a shift of the intraventricular septum. The ventricular septal shift to the left causes a left ventricular diastolic dysfunction, which further increases pulmonary hydrostatic pressures.[11]
- Neurogenic causes[12] (seizures, head trauma, strangulation, electrocution).
- Pulmonary embolism[13]
Acute lung injury may also cause pulmonary edema through injury to the vasculature and parenchyma of the lung. Acute lung injury and acute respiratory distress syndrome.[14] (ALI-ARDS) cover many of these causes, but they may include:
- Inhalation of hot or toxic gases
- Pulmonary contusion, i.e., high-energy trauma (e.g. vehicle accidents)
- Aspiration, e.g., gastric fluid
- Reexpansion, i.e. post large volume thoracocentesis, resolution of pneumothorax, post decortication, removal of endobronchial obstruction, effectively a form of negative pressure pulmonary oedema.
- Reperfusion injury, i.e. postpulmonary thromboendartectomy or lung transplantation
- Swimming induced pulmonary edema also known as immersion pulmonary edema[15][16]
- Transfusion Associated Circulatory Overload (TACO) occurs when multiple blood transfusions or blood-products (plasma, platelets, etc.) are transfused over a short period of time.[17]
- Transfusion associated Acute Lung Injury (TRALI) is a specific type of blood-product transfusion injury that occurs when the donors plasma contained antibodies against the recipient,such as anti-HLA or anti-neutrophil antibodies.[18]
- Severe infection or inflammation which may be local or systemic. This is the classical form of ALI-ARDS.
Some causes of pulmonary edema are less well characterised and arguably represent specific instances of the broader classifications above.
- Arteriovenous malformation
- Hantavirus pulmonary syndrome
- High altitude pulmonary edema (HAPE)[19][20]
- Envenomation, such as with the venom of Atrax robustus[21]
Flash pulmonary edema
Flash pulmonary edema (FPE), is rapid onset pulmonary edema. It is most often precipitated by acute myocardial infarction or mitral regurgitation, but can be caused by aortic regurgitation, heart failure, or almost any cause of elevated left ventricular filling pressures. Treatment of FPE should be directed at the underlying cause, but the mainstays are nitroglycerin, ensuring adequate oxygenation with non-invasive ventilation, and decrease of pulmonary circulation pressures.[22]
Recurrence of FPE is thought to be associated with hypertension[23] and may signify renal artery stenosis.[24] Prevention of recurrence is based on managing hypertension, coronary artery disease, renovascular hypertension, and heart failure.
Diagnosis
There is no single test for confirming that breathlessness is caused by pulmonary edema – there are many causes of shortness of breath.
Low oxygen saturation and disturbed arterial blood gas readings support the proposed diagnosis by suggesting a pulmonary shunt. A chest X-ray will show fluid in the alveolar walls, Kerley B lines, increased vascular shadowing in a classical batwing peri-hilum pattern, upper lobe diversion (increased blood flow to the superior parts of the lung), and possibly pleural effusions. In contrast, patchy alveolar infiltrates are more typically associated with noncardiogenic edema[7]
Lung ultrasound, employed by a healthcare provider at the point of care, is also a useful tool to diagnose pulmonary edema; not only is it accurate, but it may quantify the degree of lung water, track changes over time, and differentiate between cardiogenic and non-cardiogenic edema.[25]
Especially in the case of cardiogenic pulmonary edema, urgent echocardiography may strengthen the diagnosis by demonstrating impaired left ventricular function, high central venous pressures and high pulmonary artery pressures.
Blood tests are performed for electrolytes (sodium, potassium) and markers of renal function (creatinine, urea). Liver enzymes, inflammatory markers (usually C-reactive protein) and a complete blood count as well as coagulation studies (PT, aPTT) are also typically requested. B-type natriuretic peptide (BNP) is available in many hospitals, sometimes even as a point-of-care test. Low levels of BNP (<100 pg/ml) suggest a cardiac cause is unlikely.[7]
-

Acute pulmonary edema
-

Acute pulmonary edema
-
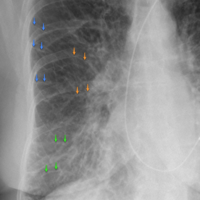
Acute pulmonary edema
-
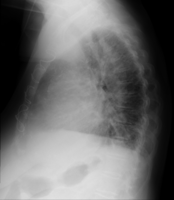
Acute pulmonary edema lateral
-
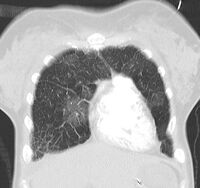
Acute pulmonary edema on CT
-

X-Ray showing pulmonary oedema
-

Pulmonary edema on CT-scan (coronal MPR)
.jpg)
.jpg)
.png)
.png)
.jpg)


Prevention
In those with underlying heart disease, effective control of congestive symptoms prevents pulmonary edema.[citation needed]
Dexamethasone is in widespread use for the prevention of high altitude pulmonary edema. Sildenafil is used as a preventive treatment for altitude-induced pulmonary edema and pulmonary hypertension,[26][27] the mechanism of action is via phosphodiesterase inhibition which raises cGMP, resulting in pulmonary arterial vasodilation and inhibition of smooth muscle cell proliferation.[28] While this effect has only recently been discovered, sildenafil is already becoming an accepted treatment for this condition, in particular in situations where the standard treatment of rapid descent has been delayed for some reason.[29]
Management
The initial management of pulmonary edema, irrespective of the type or cause, is supporting vital functions. Therefore, if the level of consciousness is decreased it may be required to proceed to tracheal intubation and mechanical ventilation to prevent airway compromise. Low oxygen levels may require supplementary oxygen, but if this is insufficient then again mechanical ventilation may be required to prevent complications.[citation needed] Treatment of the underlying cause is the next priority; pulmonary edema secondary to infection, for instance, would require the administration of appropriate antibiotics.[citation needed]
Cardiogenic
Acute cardiogenic pulmonary edema often responds rapidly to medical treatment.[30] Positioning upright may relieve symptoms. A loop diuretic such as furosemide is administered, often together with morphine to reduce respiratory distress.[30] Both diuretic and morphine may have vasodilator effects, but specific vasodilators may be used (particularly intravenous glyceryl trinitrate or ISDN) provided the blood pressure is adequate.[30]
Continuous positive airway pressure and bilevel positive airway pressure (BIPAP/NIPPV) has been demonstrated to reduce mortality and the need of mechanical ventilation in people with severe cardiogenic pulmonary edema.[31]
It is possible for cardiogenic pulmonary edema to occur together with cardiogenic shock, in which the cardiac output is insufficient to sustain an adequate blood pressure. This can be treated with inotropic agents or by intra-aortic balloon pump, but this is regarded as temporary treatment while the underlying cause is addressed.[30]
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 1.15 1.16 Malek, R; Soufi, S (January 2020). "Pulmonary Edema". PMID 32491543.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ 2.0 2.1 Dobbe, L; Rahman, R; Elmassry, M; Paz, P; Nugent, K (December 2019). "Cardiogenic Pulmonary Edema". The American journal of the medical sciences. 358 (6): 389–397. doi:10.1016/j.amjms.2019.09.011. PMID 31813466.
- ↑ 3.0 3.1 Clark, SB; Soos, MP (January 2020). "Noncardiogenic Pulmonary Edema". PMID 31194387.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ 4.0 4.1 Medical Terminology Made Incredibly Easy!. Lippincott Williams & Wilkins. 2008. p. 160. ISBN 978-0-7817-8845-8. Archived from the original on 2021-08-29. Retrieved 2021-02-23.
- ↑ Gallin, John I.; Ognibene, Frederick P. (2012). Principles and Practice of Clinical Research. Academic Press. p. 2. ISBN 978-0-12-382168-3. Archived from the original on 2021-08-29. Retrieved 2021-02-23.
- ↑ Boron, Walter F.; Boulpaep, Emile L. (2012). Medical Physiology, 2e Updated Edition E-Book: with STUDENT CONSULT Online Access. Elsevier Health Sciences. p. 493. ISBN 978-1-4557-1181-9. Archived from the original on 2021-08-29. Retrieved 2021-02-23.
- ↑ 7.0 7.1 7.2 Ware LB, Matthay MA (December 2005). "Clinical practice. Acute pulmonary edema". N. Engl. J. Med. 353 (26): 2788–96. doi:10.1056/NEJMcp052699. PMID 16382065.
- ↑ What Is Pulmonary Hypertension? Archived 2012-04-27 at the Wayback Machine From Diseases and Conditions Index (DCI). National Heart, Lung, and Blood Institute. Last updated September 2008. Retrieved on 6 April 2009.
- ↑ Adair, Olivia Vynn (2001). Cardiology secrets (2nd ed.). Elsevier Health Sciences,. Chapter 41, page 210. ISBN 1-56053-420-6. Archived from the original on 2016-05-29. Retrieved 2016-03-13.
{{cite book}}: CS1 maint: extra punctuation (link) - ↑ Papaioannou V, Terzi I, Dragoumanis C, Pneumatikos I (2009). "Negative-pressure acute tracheobronchial hemorrhage and pulmonary edema". J Anesth. 23 (3): 417–20. doi:10.1007/s00540-009-0757-0. PMID 19685125.
- ↑ Hines, Roberta L. and Marschall, Katherine. Stoelting's Anesthesia and Co-Existing Disease. 6th edition. 2012. pages 178 and 179.
- ↑ O'Leary, R.; McKinlay, J. (2011). "Neurogenic pulmonary oedema". Continuing Education in Anaesthesia, Critical Care & Pain. 11 (3): 87–92. doi:10.1093/bjaceaccp/mkr006. Archived from the original on 2020-08-14. Retrieved 2019-12-16.
- ↑ "Pulmonary edema". Mayo Clinic. 2018-08-08. Archived from the original on 2020-02-22. Retrieved 2020-03-11.
- ↑ Boyle, AJ; Mac Sweeney, R; McAuley, DF (August 2013). "Pharmacological treatments in ARDS; a state-of-the-art update". BMC Med. 11: 166. doi:10.1186/1741-7015-11-166. PMC 3765621. PMID 23957905.
- ↑ Hampson NB, Dunford RG (1997). "Pulmonary edema of scuba divers". Undersea Hyperb Med. 24 (1): 29–33. PMID 9068153. Archived from the original on 2010-06-17. Retrieved 2008-09-04.
- ↑ Cochard G, Arvieux J, Lacour JM, Madouas G, Mongredien H, Arvieux CC (2005). "Pulmonary edema in scuba divers: recurrence and fatal outcome". Undersea Hyperb Med. 32 (1): 39–44. PMID 15796313. Archived from the original on 2011-01-17. Retrieved 2008-09-04.
- ↑ "Adverse Reactions". Professional Education. 2016-06-02. Archived from the original on 2016-12-20. Retrieved 2016-12-03.
- ↑ "Transfusion-related acute lung injury (TRALI)". Professional Education. 2016-06-17. Archived from the original on 2016-12-20. Retrieved 2016-12-03.
- ↑ Luks AM (2008). "Do we have a "best practice" for treating high altitude pulmonary edema?". High Alt. Med. Biol. 9 (2): 111–4. doi:10.1089/ham.2008.1017. PMID 18578641.
- ↑ Bates, M (2007). "High altitude pulmonary edema". Altitude Physiology Expeditions. Archived from the original on 2010-01-09. Retrieved 2008-09-04.
- ↑ White J, Gray M, Fisher M (1989). Atrax Robustus Archived 2014-04-02 at the Wayback Machine IPCS InChem
- ↑ Long, Brit; Koyfman, Alex; Gottlieb, Michael (2018). "Management of Heart Failure in the Emergency Department Setting: An Evidence-Based Review of the Literature". The Journal of Emergency Medicine. 55 (5): 635–646. doi:10.1016/j.jemermed.2018.08.002. PMID 30266198.
- ↑ Kramer K, Kirkman P, Kitzman D, Little WC. Flash pulmonary edema: association with hypertension and recurrence despite coronary revascularization. Am Heart J. 2000 Sep;140(3):451–5. doi:10.1067/mhj.2000.108828. PMID 10966547.
- ↑ Pickering TG, Herman L, Devereux RB, Sotelo JE, James GD, Sos TA, Silane MF, Laragh JH. Recurrent pulmonary oedema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularisation. Lancet. 1988;332(8610):551–2. doi:10.1016/S0140-6736(88)92668-2. PMID 2900930.
- ↑ Volpicelli, Giovanni; Elbarbary, Mahmoud; Blaivas, Michael; Lichtenstein, Daniel A.; Mathis, Gebhard; Kirkpatrick, Andrew W.; Melniker, Lawrence; Gargani, Luna; Noble, Vicki E. (2012-04-01). "International evidence-based recommendations for point-of-care lung ultrasound". Intensive Care Medicine. 38 (4): 577–591. doi:10.1007/s00134-012-2513-4. ISSN 1432-1238. PMID 22392031.
- ↑ Richalet JP, Gratadour P, Robach P, et al. (2005). "Sildenafil inhibits altitude-induced hypoxemia and pulmonary hypertension". Am. J. Respir. Crit. Care Med. 171 (3): 275–81. doi:10.1164/rccm.200406-804OC. PMID 15516532.
- ↑ Perimenis P (2005). "Sildenafil for the treatment of altitude-induced hypoxaemia". Expert Opin Pharmacother. 6 (5): 835–7. doi:10.1517/14656566.6.5.835. PMID 15934909.
- ↑ Clark, Michael; Kumar, Parveen J. (2009). Kumar and Clark's clinical medicine. St. Louis, Mo: Elsevier Saunders. p. 783. ISBN 978-0-7020-2993-6.
- ↑ Fagenholz PJ, Gutman JA, Murray AF, Harris NS (2007). "Treatment of high altitude pulmonary edema at 4240 m in Nepal". High Alt. Med. Biol. 8 (2): 139–46. doi:10.1089/ham.2007.3055. PMID 17584008.
- ↑ 30.0 30.1 30.2 30.3 Cleland JG, Yassin AS, Khadjooi K (2010). "Acute heart failure: focusing on acute cardiogenic pulmonary oedema". Clin Med. 10 (1): 59–64. doi:10.7861/clinmedicine.10-1-59. PMC 4954483. PMID 20408310.
- ↑ Wang, Y; Brown, J; Godfrey, C; Ahmad, M; Vital, FMR; Lambiase, P; Banerjee, A; Bakhai, A; Chong, M. "Non‐invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema". Cochrane Database of Systematic Reviews (4): CD005351. doi:10.1002/14651858.CD005351.pub4. PMID 30950507.
External links
| Classification | |
|---|---|
| External resources |
- Pages with script errors
- CS1 errors: missing periodical
- Webarchive template wayback links
- CS1 maint: extra punctuation
- Articles containing Ancient Greek (to 1453)-language text
- All articles with unsourced statements
- Articles with unsourced statements from February 2013
- Articles with invalid date parameter in template
- Articles with unsourced statements from October 2013
- Medical emergencies
- Respiratory diseases principally affecting the interstitium
- RTT